


Wrist Fractures
Hand and wrist fractures usually occur as a result of a fall onto the hand. Some cases of hand injury happen as a result of striking a hard object, such as a wall, door, or another person. These are among the most common fractures a person can have.
The wrist is made up of several bones. It is a joint created by the connection of 8 small bones in the wrist itself and two forearm bones called the radius and ulna. All of these bones come together to make several small and a few large joints. Because the small bones are so small and often globular in shape, they rarely fracture. The most commonly fractured bones in the wrist are the larger radius and ulna, and the smaller navicular bone in the wrist.
Common scenarios for getting a wrist fracture include a car accident, a fall from a roof or ladder, or a fall on ice. If a person suffers from osteoporosis, they are more likely to sustain a wrist injury in an accident or fall.
The radius is the most commonly injured bones in the wrist. It is the long bone that makes up the forearm. This fracture can be displaced or non-displaced. A special type of fracture of the radius is called a Colles fracture. It involves a fracture of the distal radius in which the distal fragment has tipped posteriorly, leaving an obvious deformity of the wrist. It can be treated conservatively following closed reduction of the tipped fragment and casting that leaves the wrist bent forward.
Fractures of the wrist can be completely stable with all the bone fragments lining up the way they are supposed to. They can also be unstable, with the bony fragments likely to shift or tip. Unstable fractures often show a deformity of the wrist. Fractures can be closed, with no break in the skin, or open, with a piece of bone sticking out or a laceration overlying the fracture site. Open fractures carry the risk of infection in the bones or tissues. If the bones heal in an unnatural position, there can be permanent arthritis and pain of the affected wrist.
Risk fractures to a broken wrist include participation in sports, especially snowboarding, football, soccer, rugby, basketball, wrestling, hockey, in-line skating, or skiing. Older people with osteoporosis have fragile bones that easily break, even when falling from a standing position. People with bone diseases or calcium deficiency are at greater risk for wrist fractures.
A fractured wrist needs to be reduced into its proper position and treated with casting or surgery as soon as possible. If the bones do not heal in the proper alignment, it can affect your ability to grab things, write, or button your shirt. Early treatment can minimize secondary stiffness and pain.
Symptoms of a broken wrist include severe pain in the affected area and upon flexing or extending the wrist. There will be these other symptoms:
• Swelling at the site of the fracture.
• Tenderness to palpation of the wrist.
• Bruising over the fracture site.
• An obvious deformity of the wrist.
• Inability to flex, extend, pronate or supinate the wrist.
• Numb feelings or cold feelings in the hand.
Imaging studies can be used to identify where the fracture or fractures are and to tell if the fractures are in the right place or out of place. These include:
• X-rays. Plain film x-rays can visualize most cases of wrist fractures. If the bones are just cracked, however, the plain film x-ray may not reveal the presence of the fracture. Even so, they are the first line of inquiry into the presence of a wrist fracture.
• CT scan. A CT scan can easily uncover wrist fractures otherwise missed by plain film x-ray. It creates cross-sectional images of the body and can show detail not seen by other means.
• MRI scan. This uses a strong magnet and radio waves to create a cross-sectional image of bones. This technique is able to detect very tiny fractures and any ligamentous injuries that might be present.
• Bone scan. A bone scan uses an injected amount of radioactive material in order to show up areas where the bone is just cracked and is not displaced in any way. Areas where bone is healing can also show up on an MRI scan.
In the treatment of the fractured wrist, the first job is to align the bones in their proper position. It can be done under local anesthesia and sedation or it can be done under general anesthesia.
After the bone is in its proper place, a cast or splint is used to keep the bones the way they’re supposed to be. Such casting or splinting usually takes 6 weeks before the bones heal.
The doctor may prescribe nonsteroidal anti-inflammatory medications to ease the pain and inflammation of the fracture. These include ibuprofen and naproxen, as well as COX-2 inhibitors like Celebrex. In the early stages, a narcotic pain reliever might be used to ease the initial severe pain.
After the cast or splint is removed, you may be instructed to go to physical therapy where they can teach you exercises that will improve your range of motion and the strength of the wrist and hand.
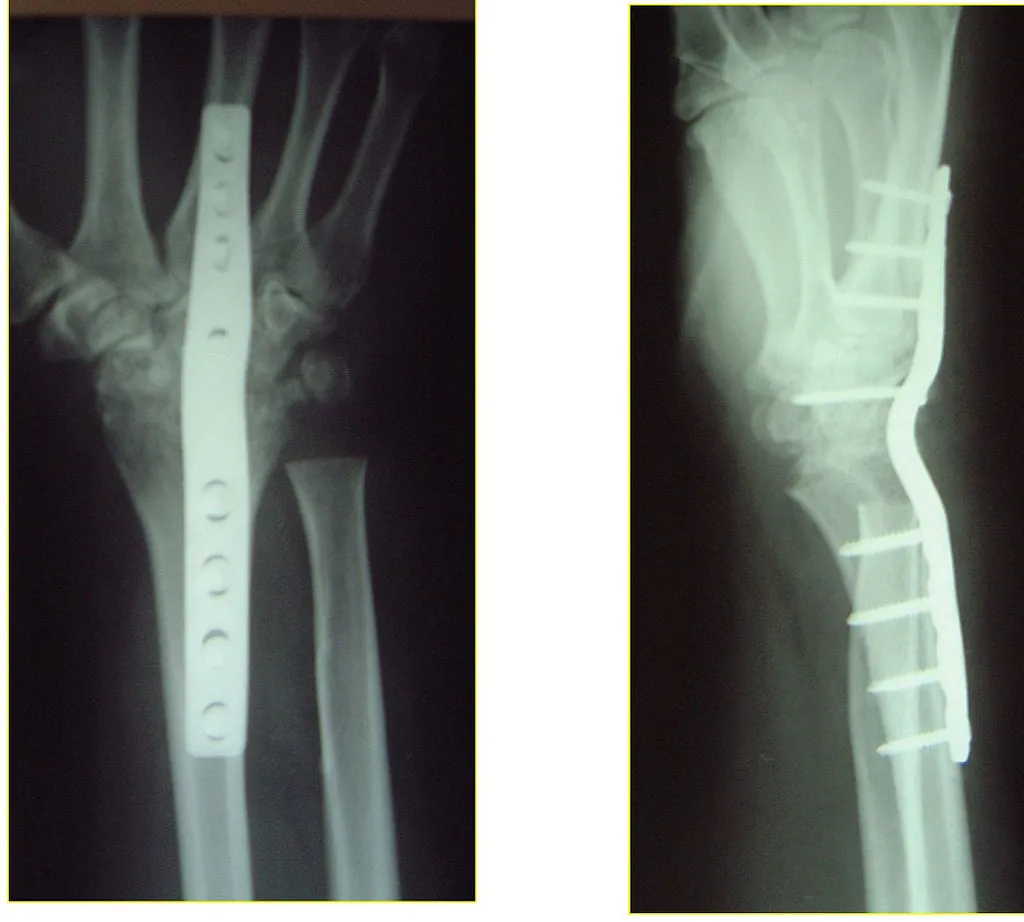 Surgery is indicated in certain situations. In surgery, the doctor uses plates, screws, rods, or bone grafts to align and fix the bones in the right position. This is called internal fixation. Internal fixation is done under the following circumstances:
Surgery is indicated in certain situations. In surgery, the doctor uses plates, screws, rods, or bone grafts to align and fix the bones in the right position. This is called internal fixation. Internal fixation is done under the following circumstances:
• The presence of multiple fractures
• The presence of loose bone fragments that could go into a joint
• An unstable fracture
• A fracture that is displaced
• Fractures that go into a joint
• A fracture that involves crushing of the bone
Complications of a wrist fracture include having an ongoing disability with stiffness and aching of the wrist. While it can occur normally in the first few weeks after the cast is removed, ongoing stiffness and pain is not normal after that. You can also get osteoarthritis of the joint, especially if the fracture extended into the joint. In some cases, you can get blood vessel or nerve damage from the trauma to your wrist.
Navicular Fracture
The navicular bone is also called the scaphoid bone. It is the most commonly fractured bone in the wrist. It is one of eight carpal bones located in the wrist. The navicular bone is usually fractured when the bone is pushed up against the radius. It happens with a fall in which the palm of the hand broke the fall and the arm was outstretched. The wrist is hyperextended, pinching the navicular bone in half until it fractures.
Common symptoms of this type of fracture include pain in the wrist and tenderness over the “anatomical snuffbox”, located on the thumb side of the wrist. It is difficult to pick up a navicular fracture on plain film x-ray. If there is clinical evidence of a navicular fracture without x-ray evidence, a bone scan can pick up the fracture.
It is vital that the navicular fracture is diagnosed as early as possible. A portion of the navicular has a very poor blood supply and a fracture can cause a breakdown of that part of the bone. Chronic arthritis can set in which it is difficult to heal. If the navicular fracture is caught in time, the blood supply can be reestablished so the bony fragments can heal. The odds that the bone heals itself without medical attention are very low.
The treatment for navicular fractures is dependent on the shape of the fracture line and the severity of the fracture. One treatment used is a long arm cast for a period of six weeks and then using a short arm cast until the bone is healed. Another treatment involves using a short arm cast for three months with the use of a rigid splint for an additional two months. It usually takes this long for this delicate type of fracture to heal.
Nondisplaced fractures with poor or no healing after 3-4 months often need surgery to fix the fracture or electrical stimulation to stimulate bone growth. If the fracture is displaced, it needs surgery. The surgery often requires the use of bone grafts and others need screws or wires to hold the navicular bone together. The person is then put into a long-arm cast for a total of six weeks followed by a short arm cast. X-rays and bone scans, along with the patient’s symptoms determine when the patient can undergo physical therapy without a cast.
Rehabilitation usually follows the period of immobilization. The patient has strengthening exercises along with improvement in range of motion and function of the wrist. The patient may need to wear some kind of splint when doing activities that stress the wrist. Exercises may need to be done for several months.
Hand Fractures
Fractures of the hand can include fractures of the metacarpals, which are located in the fleshy part of the hand. It can also include fractures of the phalanges, which are the bones of the fingers and thumb. Hand fractures can result from a crush injury to the hand, a sports injury, or a twisting injury of the hand or fingers. Because the hand is relatively small, several bones can be fractured at once, making the series of fractures more complicated to treat.
The symptoms and signs of a hand fracture include:
• Swelling at the site of the injury
• Tenderness to palpation of the fracture
• An obvious deformity of the hand
• An inability to move at least one of the fingers without pain
• A finger that is shorter than the opposite finger
• A finger that crosses over its neighboring finger
• A depressed knuckle, commonly seen in the “boxer’s fracture”.
A Boxer’s fracture is a type of hand fracture in which the individual strikes someone or something and ends up fracturing their fifth metacarpal. There is a deformity to the little finger side of the hand and an absence or depression of the knuckle. It is commonly treated with a splint along the ulnar side of the forearm and onto the hand. In some cases, it can be treated with surgery to speed healing.
The diagnosis of a hand fracture depends on a careful history and physical examination. X-rays are usually quite good at detecting hand fractures unless the fracture is just a cracked bone.
The treatment of a hand fracture involves manually relocating the bones, usually under local anesthesia and holding the bones in place with a cast that extends from the fingertips to near the elbow. X-rays are repeated about a week after the injury to make sure the bones are healing in the proper position.
In a hand fracture, the splint or cast will be worn for about 3-6 weeks. After this, x-rays are done to assure healing has taken place. After the cast is removed, the person usually begins physical therapy and rehabilitation in order to gain some range of motion of the hand and to strengthen the muscles of the hand and forearm. Complications include osteoarthritis of the hand in the area of the fracture. This occurs especially in those fractures that have gone into the joint space at the time of the injury.
Surgical treatment is necessary for some places. It is especially needed when the bony fragments are not aligned and cannot be aligned manually. Crush injuries often need to be treated with surgery. Screws, plates or wires can be used to repair the phalanges and the metacarpals. Open fractures are often treated with surgery. In some cases, the surgeon removes the hardware after the bone has healed. In other cases, it is left in the body.
Joint stiffness is a possibility after immobilizing the bone for so long. The physical therapist can recommend exercises that relieve the joint stiffness and strengthen the hand. Physical therapy can last for several weeks.
After the fracture has healed, the hand should be healed without difficulty. The two most common issues that patients with a hand fracture have are finger stiffness with no obvious deformity or osteoarthritic spurs and a noticeable bump over the fractured area. The bump usually passes over time and the stiffness of the finger can be overcome by a beginning range of motion as soon as possible after the fracture is stable.
Sacramento Personal Injury Lawyer
I’m Ed Smith, a Sacramento personal injury attorney with the primary accident information site on the web, AutoAccident.com. If you or a loved one has suffered a traumatic injury caused by the negligence of another, call me now at 916.921.6400.
You can find out more about our office by looking for us either on Yelp or on Avvo, the attorney rating site.